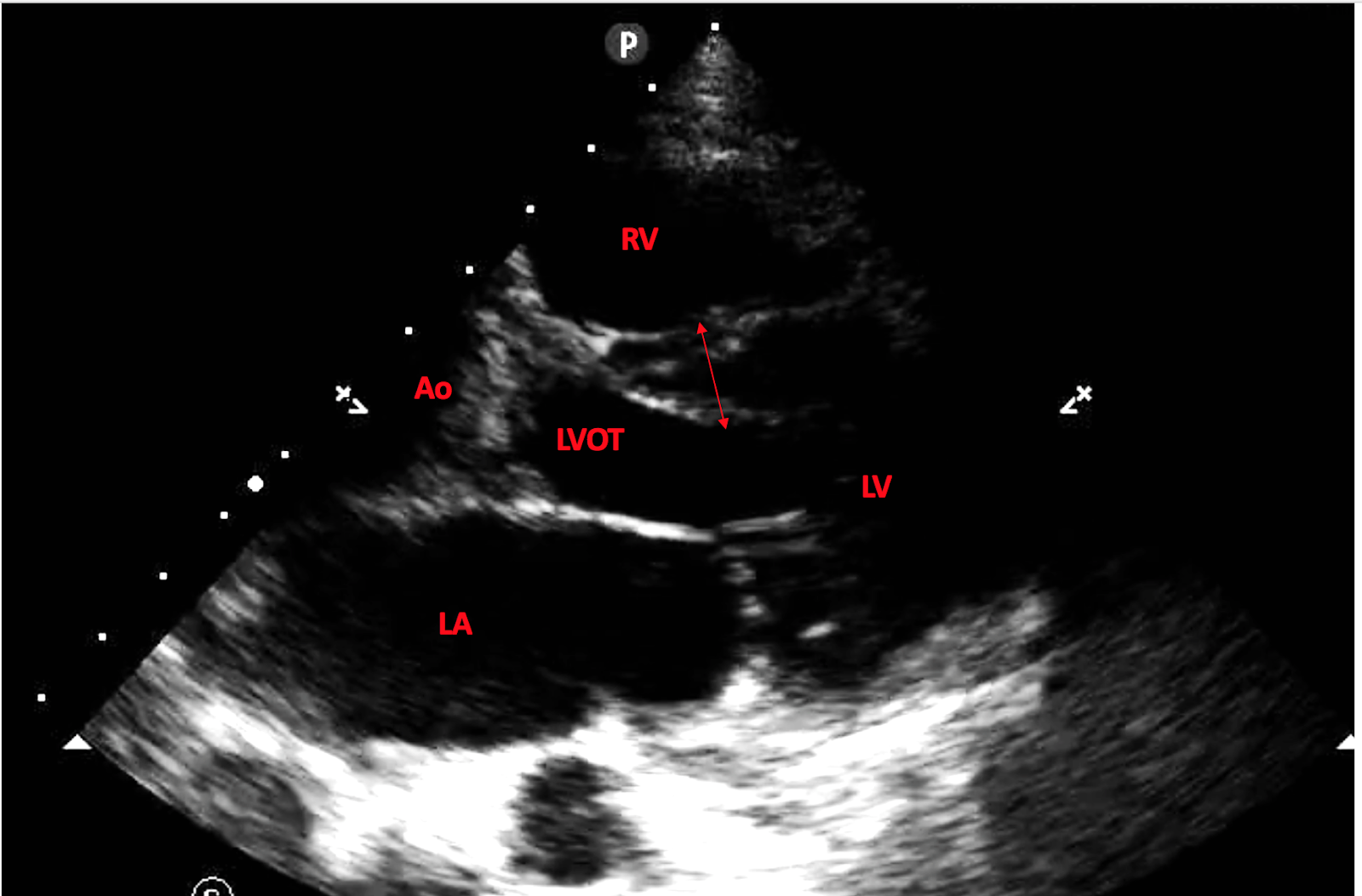
The video file, showing the parasternal long axis:
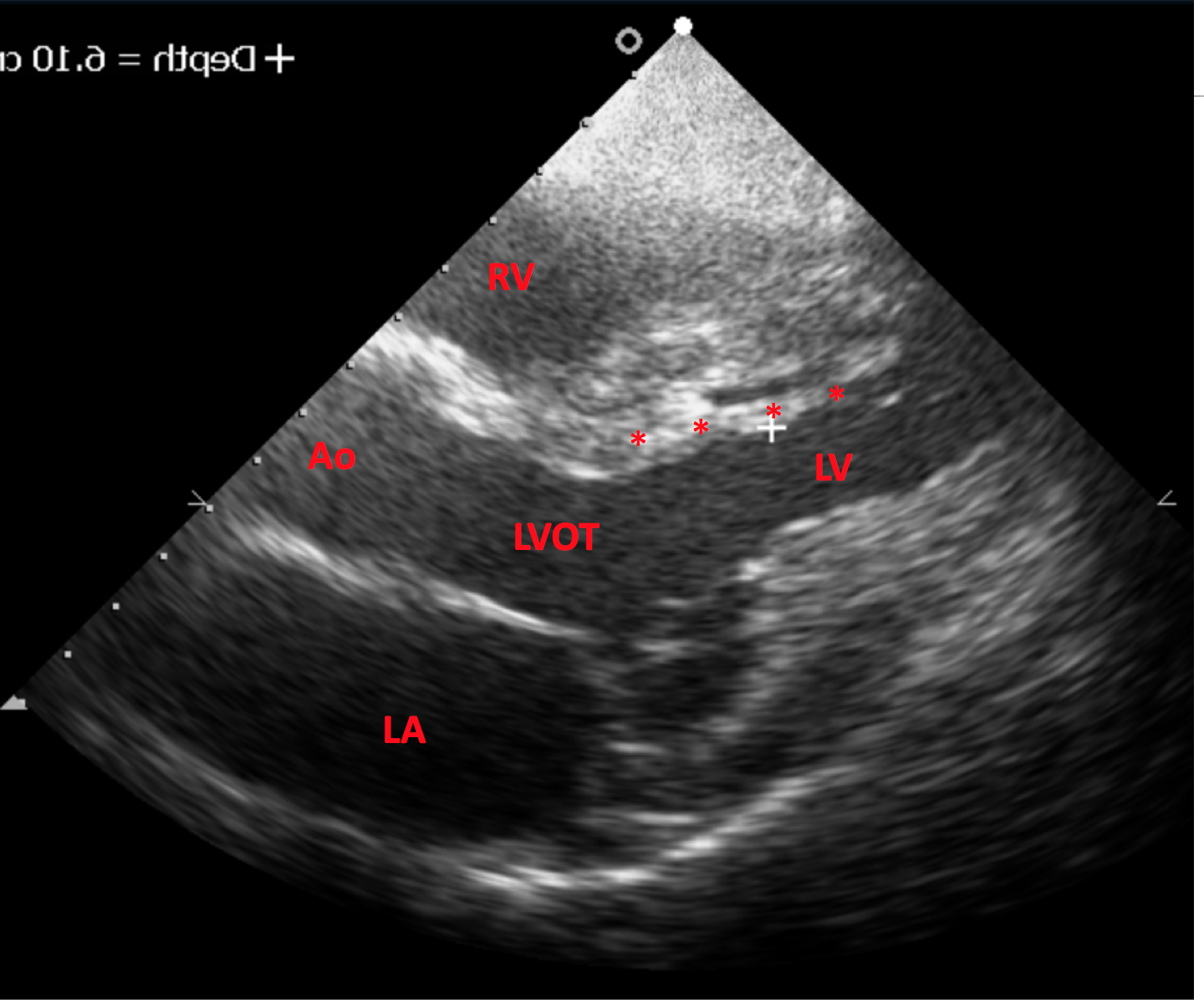
I noted that there was an echo-free space within this “septum.” Instead of a thickened septum, there seemed to be normal wall thickness, but with a linear structure attached to the basal ventricular septum (red asterisks):

This appears to be a left ventricular false tendon. Similar to the moderator band in the right ventricle, the false tendon is a benign structure which may be mistaken for pathology.
False tendons may be composed of just simple fibrous tissue, but they may also contain myocardial muscle, Purkinje fibers, or even coronary arteries ( For a clear and concise review, unfortunately paywall access.)
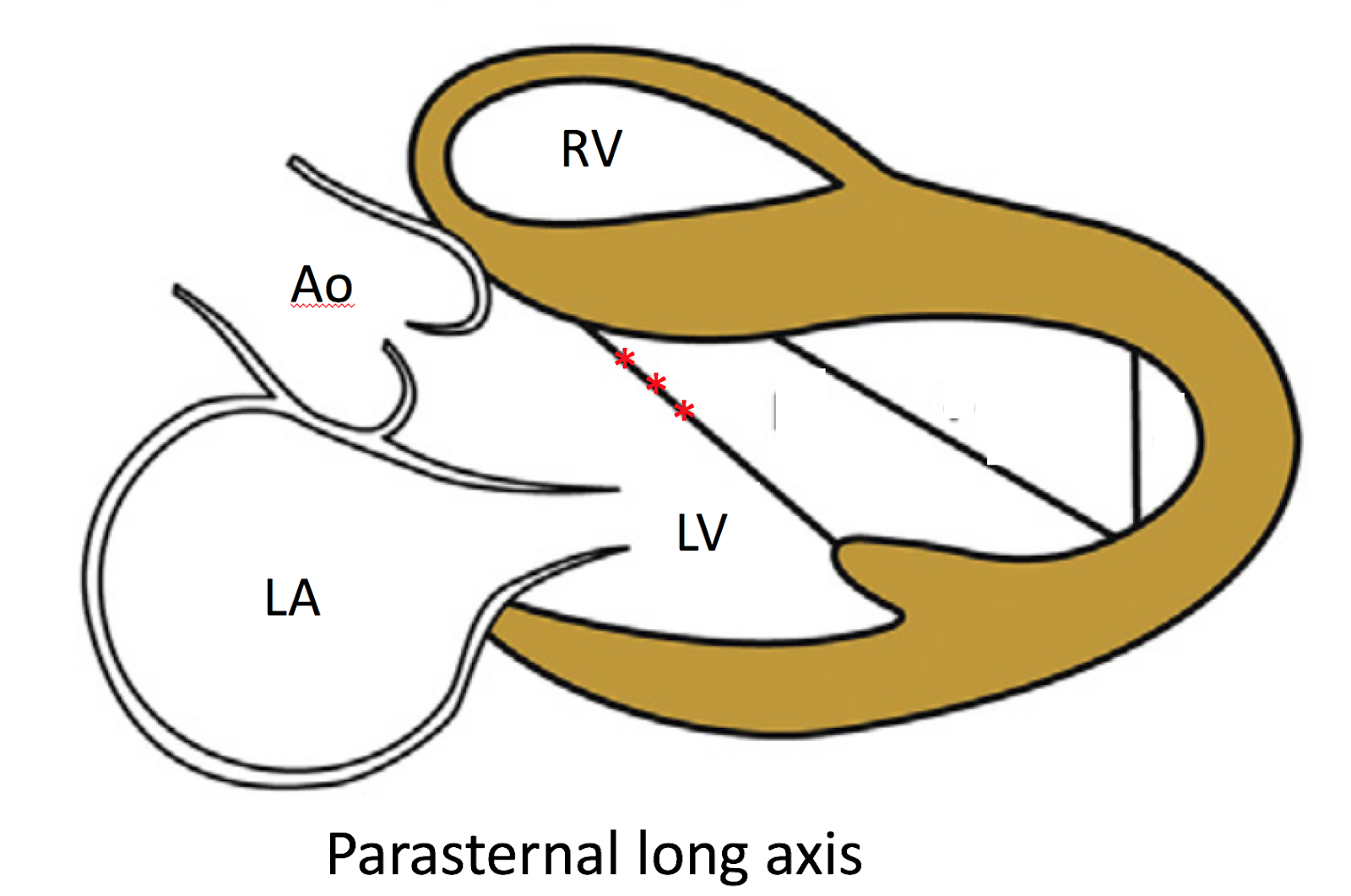
False tendons are quite common, seen in about half of autopsies, and are most common seen attached to the basal septum, running to the posteromedial papillary muscle (red asterisks, as above):
Some case reports have associated false tendons with early repolarization pattern on the ECG, episodes of ventricular arrhythmias, or with a pseudo-STEMI pattern on the ECG. To these risks of false tendons we can add the potential for incorrectly diagnosing HCM!
This has happened before. A case report by Ker described a young adult with a mild murmur who was initially thought to have septal hypertrophy demonstrated on the echocardiogram. Closer evaluation revealed, instead, a false tendon in the same location as our patient!
So, be careful with the FoCUS. Pitfalls abound when considering diagnoses beyond the entities we usually assess (e.g. effusion, aortic root, RV dilation, EF).
Open-access references:
Left ventricular false tendons and electrocardiogram repolarization abnormalities in healthy young subjects